Ashwagandha vs Rhodiola — Which Works Best for Stress?
Team Alpha
10/2/20255 min read
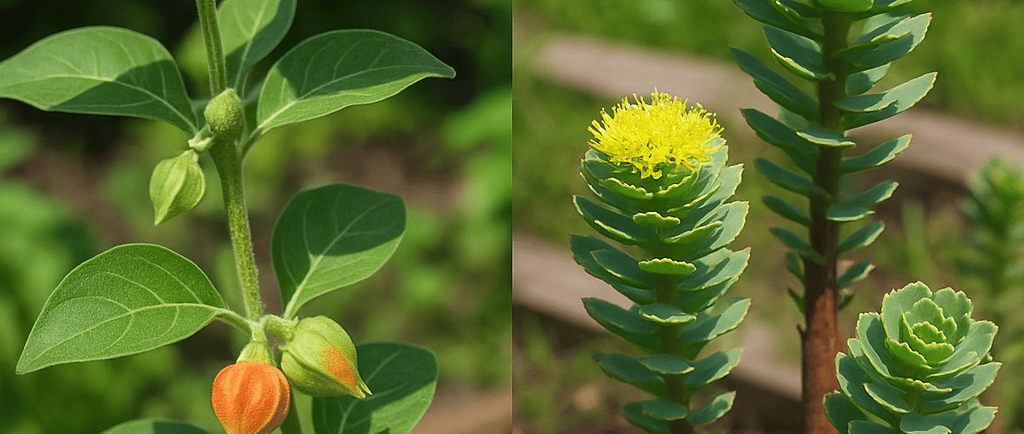

If you juggle long workdays, travel, deadlines and family, the promise of a natural supplement that eases stress, clears brain fog, and restores energy is tempting. Two of the most popular adaptogens are ashwagandha (Withania somnifera) and rhodiola (Rhodiola rosea). Both have decades of traditional use and a growing clinical literature — but they are not identical. This article walks through the science, the measurable effects (the metrics researchers use), safety, practical dosing ranges used in trials, and how to pick the right herb depending on your goals and context.
Short answer (if you don’t want the deep dive)
Ashwagandha has the stronger clinical evidence for reducing perceived stress and lowering morning cortisol in randomized controlled trials and meta-analyses — useful if your stress looks like chronic tension, anxiety or elevated cortisol. PMC+1
Rhodiola shows more consistent evidence for improving fatigue, mental stamina and stress-related burnout, especially in short-term studies of stress-related fatigue and work/exam stress. It’s often reported to increase alertness and reduce subjective fatigue. PubMed+1
Both are generally well tolerated short-term; choose based on whether your primary complaint is anxiety/elevated cortisol (ashwagandha) vs fatigue/mental stamina (rhodiola). Check drug interactions and don’t mix adaptogens with certain prescription meds without medical advice. NCCIH
How these adaptogens are measured in clinical research (the metrics to watch)
Clinical trials don’t just ask “does it work?” — they measure how it works with repeatable metrics:
Perceived Stress Scale (PSS) — a common self-report for chronic stress. Changes in PSS are widely reported in ashwagandha trials. PMC
Hamilton Anxiety Rating Scale (HAM-A) and DASS-21 — used in anxiety studies (ashwagandha trials report changes here). PubMed
Morning cortisol (serum or salivary) — objective endocrine marker of HPA-axis activation; reductions indicate biological stress mitigation. Ashwagandha trials have documented morning cortisol decreases. PubMed
Fatigue and mental performance scales (e.g., MFI, clinical fatigue scales) — often used in rhodiola trials focused on stress-related fatigue and work/exam stress. PubMed+1
Adverse events and tolerability — frequency & severity recorded in every RCT; key for clinicians and executives assessing risk/benefit. NCCIH
Key clinical evidence — Ashwagandha
1. Randomized controlled trials (examples & metrics)
Chandrasekhar et al., 2012 (double-blind RCT): Adults under chronic stress taking a high-concentration full-spectrum ashwagandha root extract for 6 weeks showed statistically significant improvements on perceived stress and anxiety scales versus placebo. This paper is widely cited as early, high-quality evidence for ashwagandha’s stress-reducing effect. PMC
Lopresti et al., 2019 (8-week RCT): Found reduction in morning cortisol (P < .001) and improvement in anxiety scores. Objective cortisol reduction is powerful because it shows an endocrine change, not just subjective feeling. PubMed
2. Meta-analysis & systematic reviews
A recent dose-response meta-analysis and systematic review of randomized trials concluded that ashwagandha supplementation produces significant reductions in stress and anxiety scores across studies, supporting a moderate clinical effect size (multiple RCTs pooled). These reviews also highlight heterogeneity in extracts/dosing and call for more large trials. PubMed+1
3. Typical dosing in trials
Commonly studied doses: 300–600 mg/day of standardized root extract (often given as 300 mg twice daily or 600 mg once daily) for 6–12 weeks. Cortisol reductions and PSS improvements were reported in that range. PMC+1
4. Safety
Short-term trials report good tolerability; adverse events are generally mild (GI upset, drowsiness rarely). The NIH Office of Dietary Supplements summarizes trial evidence and safety notes. Still, people on sedatives, thyroid meds, or immunosuppressants should use caution and consult a clinician. Office of Dietary Supplements+1
Bottom line for ashwagandha: Best evidence for lowering perceived stress and cortisol — a good first choice if your main problem is chronic anxiety, feeling wired, or physiological signs of HPA-axis overdrive.
Key clinical evidence — Rhodiola
1. Randomized controlled trials (examples & metrics)
Olsson et al., 2009 (SHR-5 extract, RCT): Participants with stress-related fatigue had significant improvement in fatigue and mental performance measures with rhodiola extract versus placebo; study used validated fatigue scales and cognitive endpoints. PubMed
Early Russian and Scandinavian trials (Spasov, Darbinyan) showed reduced exam-stress fatigue and improved attention under acute stress — these formed the backbone for modern rhodiola research. ScienceDirect+1
2. Systematic reviews & recent analyses
Reviews in the last decade describe consistent findings for reduced fatigue and improved mental performance, though they also note variable quality across small trials and recommend higher-quality RCTs. A 2022 review summarized rhodiola’s adaptogenic effects on fatigue and stress resilience. PMC+1
3. Typical dosing
Trials use a broad dose range: 200–600 mg/day of standardized rhodiola root extract (often SHR-5 or similar). Effective short regimens (2–4 weeks) are common in exam or work stress studies; some research uses up to 12 weeks for fatigue syndromes. PubMed+1
4. Safety & interactions
Rhodiola is generally considered safe for short-term use (up to 12 weeks) but reported side effects include dizziness, headache, insomnia and rarely GI symptoms. Rhodiola can interact with some hypertensive drugs and may theoretically affect serotonergic medications — consult a clinician before combining with SSRIs or blood-pressure agents. The US NCCIH summarizes safety signals. NCCIH+1
Bottom line for rhodiola: Choose rhodiola when fatigue and mental stamina under stress are your core issues — for short bursts of high mental demand it may be particularly useful.
How to choose, simple decision flow
Are you wired, anxious, have high morning cortisol or poor stress recovery? → Start with ashwagandha. Look for a standardized root extract and 300–600 mg/day. PMC+1
Are you exhausted, hitting mental fatigue, need stamina for intense work sprints? → Try rhodiola (200–400 mg/day), often used in short cycles during high-demand periods. PubMed+1
Both? Some users cycle or combine strategies (e.g., rhodiola in the day for energy, ashwagandha in the evening to blunt stress) — but don’t mix without checking interactions and a clinician’s advice. Evidence for combinations is limited. ScienceDirect
Safety, interactions & practical tips
Drug interactions: Ask a clinician if you’re on SSRIs, benzodiazepines, thyroid medications, immunosuppressants, or antihypertensives. Rhodiola and ashwagandha can interact or add effects. NCCIH+1
Quality matters: Use standardized extracts from reputable manufacturers; look for third-party testing. Trial results depend on standardized extracts (e.g., SHR-5 for rhodiola). PubMed
Short-term vs long-term: Most trials are short (weeks to a few months). Long-term safety data are limited; treat these as targeted tools, not lifelong prescriptions by default. NCCIH+1
Final verdict for the busy, high-performing professional
Both herbs are evidence-backed adaptogens, but they serve slightly different needs:
If your stress is primarily physiological/anxious with elevated cortisol or poor recovery: ashwagandha has the stronger, replication-level evidence for reducing stress and morning cortisol. PMC+1
If your main issue is daytime fatigue and depleted mental stamina (especially during periods of intense, time-limited demand): rhodiola is more consistently shown to reduce fatigue and support mental performance. PubMed+1
Both can be part of a science-backed toolkit for longevity, stress resilience and energy optimization — but remember lifestyle (sleep, nutrition, exercise, recovery) remains the highest-impact strategy. Supplements can complement, not replace, those foundations.
References
Chandrasekhar K, et al. Prospective, randomized, double-blind, placebo-controlled study — Ashwagandha for stress and anxiety. PubMed/PMC. PMC
Lopresti AL, et al. 2019. Randomized double-blind, placebo-controlled — Ashwagandha: reductions in morning cortisol and anxiety. PubMed. PubMed
Akhgarjand C, et al. 2022. Systematic review and dose-response meta-analysis — Ashwagandha for stress/anxiety. PubMed. PubMed
Olsson EM, et al. 2009. Randomized double-blind placebo-controlled study — Rhodiola SHR-5 for stress-related fatigue. PubMed. PubMed
Stojcheva EI, et al. 2022. Review of Rhodiola rosea — clinical evidence on fatigue/stress and mechanisms. NCBI PMC. PMC
NCCIH & NIH resources on safety and dosing summaries for rhodiola and ashwagandha. NCCIH+1
FAQ
What is the best-supported primary effect
Ashwagandha: Reduces perceived stress and morning cortisol (HPA-axis). PubMed+1
Rhodiola: Improves fatigue, mental stamina and performance under stress. PubMed+1
What was the typical trial dose given:
Ashwagandha: 300–600 mg/day (6–12 weeks). PMC
Rhodiola: 200–600 mg/day (often short course 2–4 weeks; some trials longer). PubMed
what was the objective biomarker change:
Ashwagandha: Morning cortisol reductions reported. PubMed
Rhodiola: Fewer consistent cortisol findings; primary effects often subjective fatigue/performance. ScienceDirect
Typical onset of effect:
Ashwagandha: Weeks (4–8) in most RCTs. PMC
Rhodiola: Can be quicker (days–weeks) for acute fatigue/exam stress studies. PubMed
Safety and Care notes:
Ashwagandha: Generally well tolerated; watch sedatives/thyroid meds. Office of Dietary Supplements
Rhodiola: Generally safe short-term; watch insomnia, SSRIs, BP meds. NCCIH
Insights
Expert guidance for health-conscious professionals.
Support
Connect
info@genthealthhub.com
© 2025. All rights reserved.